This leaflet is to provide you with guidance and information to help support your decisions. Carbohydrate counting involves estimating how much carbohydrate is in a meal and then calculating how much insulin will be needed for that meal.
By matching the dose of insulin to the amount of carbohydrate in a meal you can:
Improve your diabetes control (HbA1c and time in range) Stabilise your blood glucose – less highs and lows
Enjoy meals out without worrying about the effect it will have on blood glucose levels Eat big meals Eat small meals Delay or miss mealsApart from putting some time and effort in at the beginning and doing a few extra blood glucose tests, once you are up and running there aren’t really any disadvantages.
Carbohydrates are the foods that give us energy to think and be as active as we want to be. There are two main types of carbohydrate:
Please note some starchy carbohydrates have a high glycaemic index meaning they are absorbed more quickly.
*Matching rapid acting carbohydrates such as sugary drinks and jelly sweets with insulin is very difficult due to the speed at which they are absorbed. These foods and drinks should be kept for hypoglycaemia treatments only.
Some foods contain no carbohydrate or very little and therefore should not be counted.
It is important to note that although pulses (for example, lentils, chickpeas, kidney beans) contain carbohydrate this is very slowly absorbed and should not be matched with rapid acting insulin.
Baked beans are an exception due to the sugar added to the sauce. If using a food label to work out carbohydrate in your portion you can count half of the carbohydrates of beans or use the “of which sugars” value.
Most of the starches and sugars (carbohydrate) we eat appears in the blood as glucose, within 15 minutes to 2 hours after they are eaten.
We need to match this rise in glucose with the right amount of insulin.
The amount of carbohydrate in your diet determines the amount of insulin you will need – the more carbohydrate you eat the more insulin you will need.
There are a wide range of resources to help to work out the carbohydrate content of your meals.

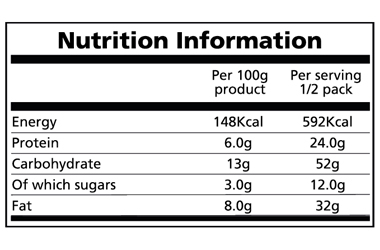
Per Serving
Here is an example of a label from a ready-made Lasagne pack size = 800g.
One serving = half the pack (400g) therefore each serving provides 52g carbohydrate
Per 100g
You can work out how much is in a serving by looking at the “per 100g” section.
The easiest way to do this is as follows:
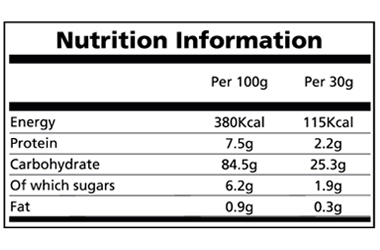
Here is a label for Rice Snaps:
Using the table right, if you were going to eat 45g you would need to:
84.5g (carbohydrate per 100g) ÷ 100 = 0.845g in 1g
0.845g x 45g (weight on scales) = 38g carbohydrate
Carbs in reference food ÷ Weight of reference food
X your Serving size = Carbs in your portions
(C ÷ W x S = Carbs)
Remember, it is the total carbohydrate number you are looking at, not the sugars or starches.
Your background insulin helps to keep your blood glucose stable overnight and between meals. To know if this dose is correct, it is important to test before bed and before breakfast. You may occasionally need to test at 3am. If the readings are within 2.0mmol/l of each other when the dose is correct. To assess this dose through the day you will need to skip a meal, have a long gap between meals or have a carbohydrate free meal.
Rapid acting insulin peaks after approximately 1 to 2 hours and lasts for approximately 4 hours. This works over the same period of time as your food is digesting. It takes 15 to 20 minutes to start working and therefore it is recommended that you count your carbohydrates and take the appropriate dose of rapid acting insulin 15 to 20 minutes before you eat where possible.
The amount of rapid acting insulin you need for each 10g of carbohydrate is called the insulin to carbohydrate ratio.
This tends to vary from 1 unit of insulin per 10g carbohydrate (which would be written as 1:10) to 3 units per 10g carbohydrate. This ratio will be worked out for you initially, but you may need to change it. Ratios should only be altered by a half unit (e.g. 1:10g would go to 1.5:10g).
The ratio may differ at different meals as many people need more insulin early in the morning. You will learn the skills to change the ratio yourself. Ratios may sometimes be altered by changing the grams of carbohydrate rather than the units of insulin (for example, 2:10g = 1:5g).
Test your blood glucose before meals to see if the dose of insulin given at the previous meal was correct.
If your blood glucose level is within 2.0mmol/l of the previous reading then the ratio is correct. If it is higher then you need more insulin with the previous meal. If it is lower then you need less. It would help to look for patterns over a few days rather than altering the ratio after one reading. It may be that you have estimated the carbohydrate incorrectly, or you have been exercising or drinking alcohol etc. therefore the reading will be a one off.

To begin with, use 1 unit per 10g carbohydrate for snacks and supper. When you are more comfortable with carbohydrate counting you can adjust this.
Snacks which are 10g of carbohydrate or less do not require any insulin. They should only increase your blood glucose by 2.0 to 3.0mmol/l and therefore you will still be in the target range.
If your snack contains more than 10g carbohydrate your blood glucose level may rise above target. It is therefore necessary to have the equivalent insulin with these snacks. Your dietitian or diabetes nurse will discuss this with you.
If your blood glucose before a meal is above target you will need to give extra insulin on top of the amount you have worked out for your carbohydrate, to bring the blood glucose back into target.
One unit of insulin reduces your blood glucose by around 2.0 to 3.0mmol/l but this varies between individuals. This is your insulin sensitivity factor (ISF).
1 unit of rapid acting insulin reduces blood glucose by 3.0mmol/l.
Insulin for meal = 5 units
Correction dose = 3 units
Total insulin required = 8 units
If you test soon after a meal (within 4 hours) and your blood glucose level is high then do not correct with additional insulin at this point. This is because it will overlap with the previous dose of insulin and may cause a hypo later in the day. It may be that the insulin takes longer to peak in your body which results in high blood glucose soon after a meal.
If your blood glucose level is high before a meal you need to consider what may have caused this before giving a correction dose, for example’ have you had a snack?
| unit(s) per 10 grams of carbohydrate at breakfast |
| unit(s) per 10grams of carbohydrate at lunch |
| unit(s) per 10grams of carbohydrate at evening meal |